Custom Formatting
Custom Formatting allows providers to personalize how their notes are generated. By setting specific formatting instructions, you can ensure the output consistently reflects your clinical style, preferences, and workflow needs.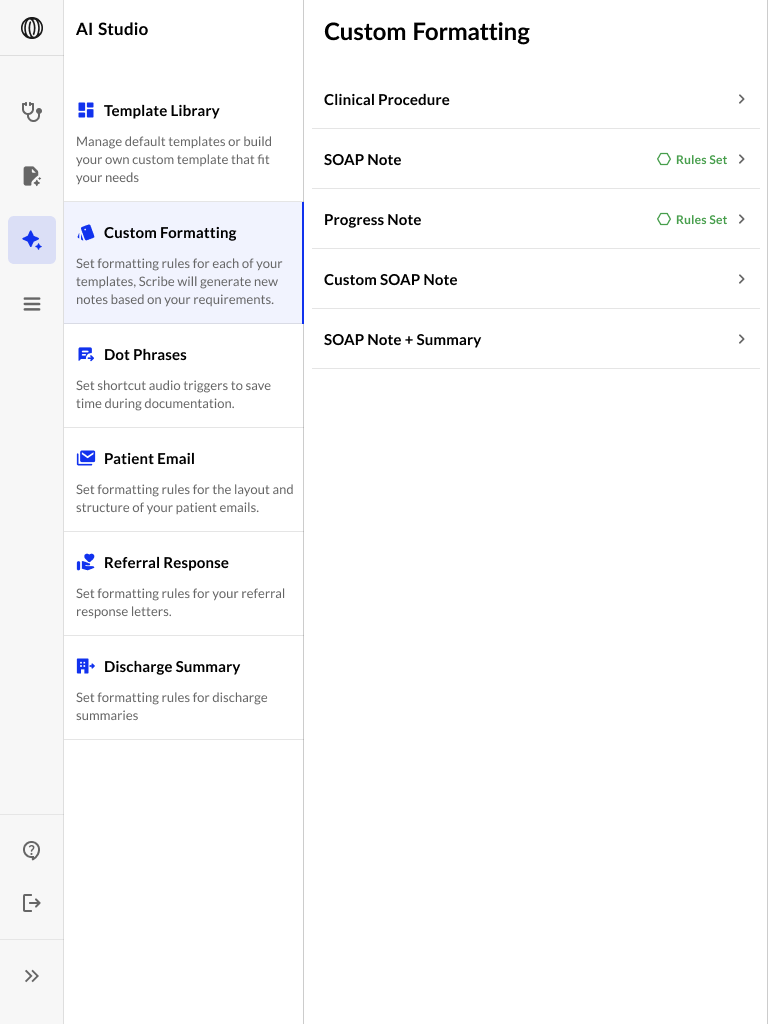
What It Does
Custom formatting applies note-by-note instructions to the AI, as if you were guiding a human scribe. These rules impact how the note is structured, phrased, and presented. For example, you can instruct the system to:- Bold all section headers
- Use bullet points in the plan
- Include gender-based salutations (e.g., “Mr” or “Mrs”)
- Number the patient’s next steps
- Add specific formatting for medications or vitals
The model will follow these instructions every time it generates a note for the selected template.
How to Set It Up
- Navigate to Custom Formatting under the AI Studio.
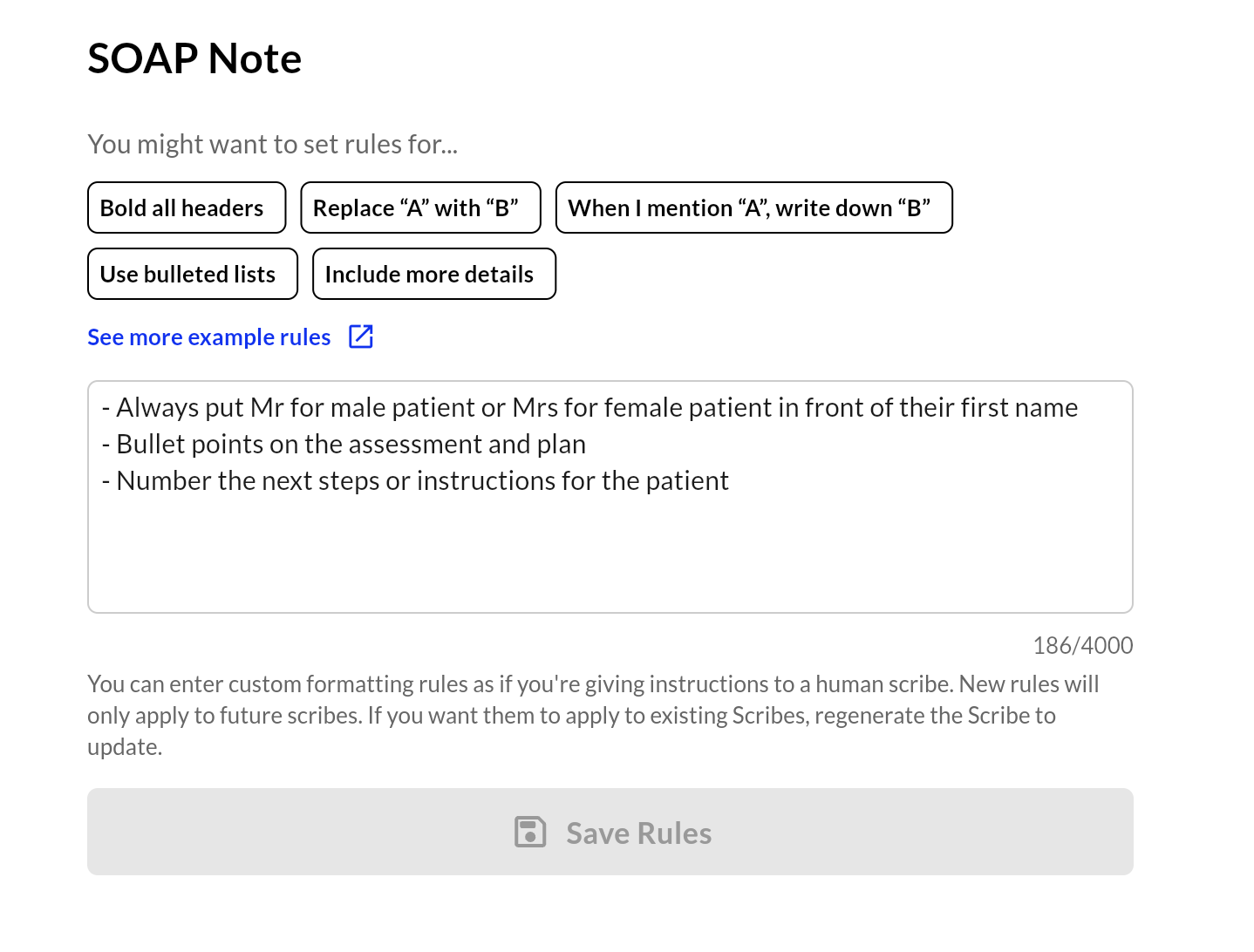
- Select the note template (e.g., SOAP Note, Progress Note).
- Use the prompt box to type your rules (up to 4,000 characters).
- Click Save Rules.
Notes
- Formatting rules only apply to future scribe generations.
- To apply updated rules to a past note, you must regenerate that note.
- Each template can have its own formatting rules—great for specialists or multi-format teams.
Examples of Useful Rules
Formatting Examples
Custom-formatting what content to include, add, or remove
- “Create a numbered problem list based on the Subjective and Objective sections.”
- “After the Assessment section, add a section called Assessment/Objective that includes a one-paragraph summary combining the Assessment and Objective sections, justifying the need for continued PT (unless the patient is to be discharged).”
- “Create a list of patient goals and/or progress toward goals based on the Subjective and Objective sections.”
- “Under the heading Neuromuscular Re-education, create a comma-separated list of all neuromuscular re-education performed.”
- “Under the heading Therapeutic Activities, create a comma-separated list of all therapeutic activities performed.”
- “Under the heading Dry Needling, create a comma-separated list of all muscles released through dry needling and/or dry needling protocols used. If electrical stimulation was used with needling, include the duration.”
- “Create the Assessment as a narrative describing what the PT did that day and how the patient responded.”
- “Always document the general exam.”
- “If I am speaking to the scribe before the start of a visit, all information discussed should be included in the documentation.”
Custom formatting writing style
- “When documenting pain levels, write them as a number out of 10 using numerals.”
- “Never write the Subjective, Objective, Assessment, or Plan in a numbered list.”
- “Refer to the patient by their name instead of ‘patient’.”
- “Never write a note in the first person.”
- “Always abbreviate physical therapy as ‘PT’.”
- “The provider addressing the patient is always the physical therapist.”
- “Refer to the PT as ‘Therapist’.”